
My project site is Jos University Teaching Hospital (JUTH). It is a tertiary hospital located in Plateau State, Nigeria. It is the seat of Stop Kernicterus and Infection in Northern Nigeria (SKIINN); a collaborative group with Jos University Teaching Hospital and their Jos partners; Ahmadu Bello University Hospital Zaria; and Aminu Kano Teaching Hospital and their partners. SKIINN’s newest project is to determine the etiologies of neonatal sepsis and antibiotic resistance patterns in neonates first in Jos and then at our other sites.
Nigeria is well-known in Sub-Saharan Africa for its high neonatal mortality rate. In 2022, its neonatal mortality rate was 34.3 deaths per 1,000 live births putting the country in the top ten leading countries for neonatal mortality worldwide. Infections such as sepsis, pneumonia, and meningitis account for a large portion of neonatal deaths with sepsis representing the top-three cause of neonatal mortality globally.
I will be going on this trip alongside 2 other residents and 4 attendings from my institution working on a longitudinal project specifically to address neonatal sepsis. I will be working on the pediatrics wards/newborn units with the local registrars, attending pediatricians, nurses and other members of the healthcare teams on the wards. During this trip, I will be engaging in bidirectional learning with the medical students, medical officers and registrars at the site through bedside teaching and formal didactics such as morning reports and case reports. Specifically using World Health Organization guidelines for training sessions. I will also be adopting phase 2 of a quality improvement project, implementing tailored hand hygiene interventions at the site.
The training during this trip will be aimed at improving knowledge and skills of the healthcare team on sepsis awareness and prevention as a tool in reduction of sepsis with the goal of improving neonatal outcomes while continuing to explore the etiologies of sepsis.
Medical students, residents, attending pediatricians, nurses and other healthcare workers at the site will benefit directly from the teachings and this will positively impact patient outcomes at the site. Most importantly, the newborn population at this site will ultimately benefit from this project.
Neonatal deaths from sepsis are highly preventable through simple cost-effective measures, such as hygienic delivery practices, cord care and exclusive breastfeeding amongst other measures. The WHO notes that for prevention of late-onset sepsis, hand washing or use of gel as hand sanitizer before contact with the patient, (after risk of exposure to biological fluids) after contact with the patient, after contact with areas near the patient, appropriate and well- define care bundles, with central intravascular catheters and endotracheal tubes that are closely followed to reduce contamination.
Trainings directed at applications of standard policies and procedures of infectious disease controls in healthcare facilities are valuable tools in neonatal sepsis prevention. In January 2024, a group of pediatricians were at JUTH for the initial phase of this project. They met with local pediatric colleagues and infection prevention specialists to identify barriers to basic interventions including hand hygiene, and to discuss some potential solutions. The visiting working group conducted an initial needs assessment as part of the first steps in addressing challenges related to prevention, diagnosis, and management of neonatal sepsis in this high incidence area in order to decrease morbidity and mortality. I will continue this ongoing work with the rest of our traveling group during my trip.
Our group met with the staff on site and discussed infection prevention at the JUTH site using WHO guidelines during the earlier visit in January 2024. I will also participate in similar lectures to reinforce previous learnings and help address ongoing questions since the previous training. The team collectively will continue to collect data to understand bacterial, viral, fungal and parasitic and antibiotic resistance patterns in neonates with sepsis. I will participate in evaluation of ongoing data and results from the project so far. I will also be adopting the second phase of a related quality improvement project that will implement tailored hand hygiene interventions at the site and set the stage for the final phase of the project that will entail a single-blinded observation to assess the effectiveness of the interventions.
As a team, we expect to continue to have greater understanding of the specific challenges around high incidence, morbidity, and mortality of neonatal sepsis in the Jos region of Nigeria. This will help us in designing customized projects to help mitigate the identified challenges and ultimately improve neonatal outcomes. I expect that our findings and lessons learned from the JUTH project can be applicable to other sites in Nigeria as well as other low middle income countries in Sub-Saharan Africa and globally.



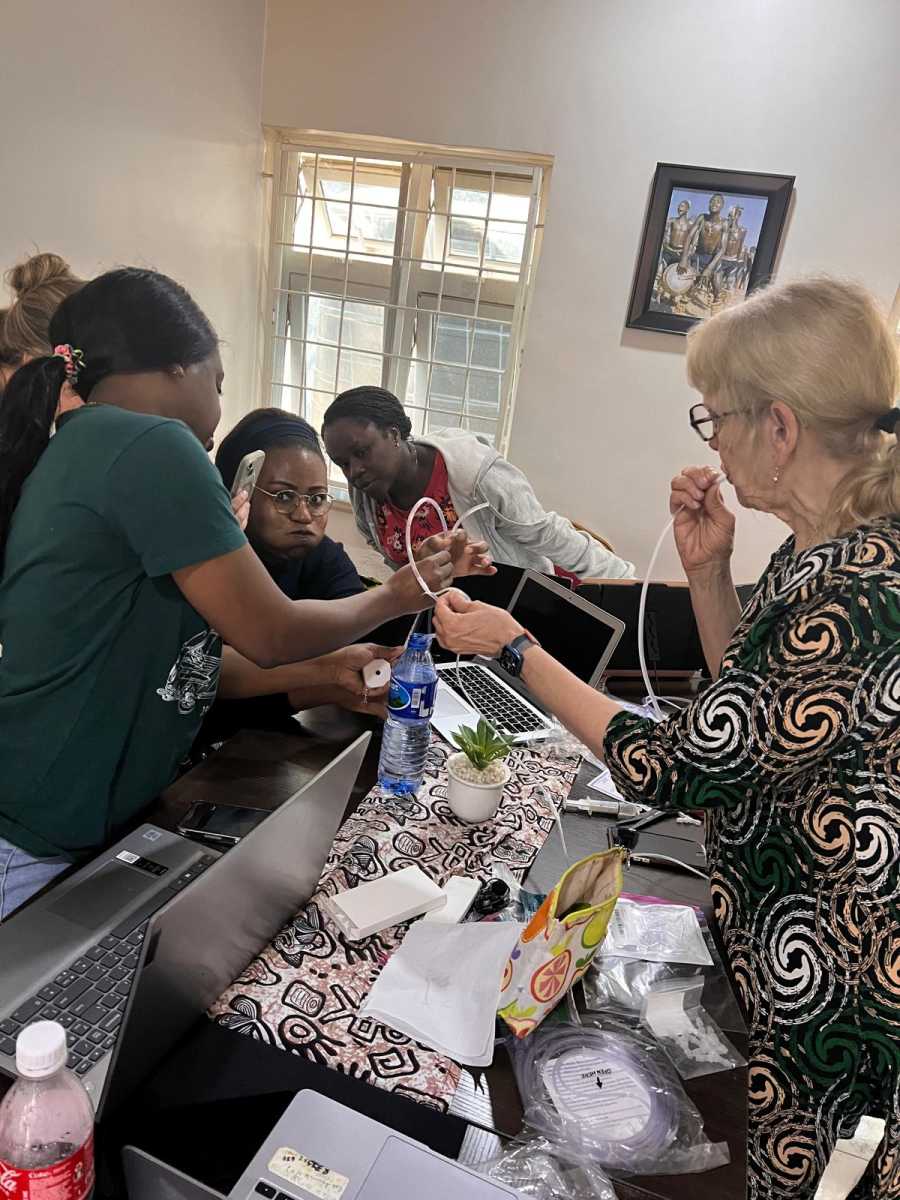






The projects I undertook in the Special Care Baby Unit— educating and training JUTH SCBU staff on the setup and utilization of low-cost bCPAP and a low-cost manometer; participating in multiple feasibility meetings to assess potential challenges and roadblocks that may arise with various sepsis modality prevention including handwashing, laboratory setup and antimicrobial stewardship. Another project I undertook was a comprehensive review of medical records in the EPU to identify and analyze the five most frequently encountered cases. The next phase of the project will involve developing a clinical protocol for the 5 most commonly encountered cases in the Emergency Pediatric Unit (EPU) at JUTH.
The most important people impacted by my projects were patients and their families. Preterms are at increased risk of respiratory failure and death but with the appropriate use of low-cost bCPAP, they have a higher chance of survival. Also, for many parents, the SCBU experience is filled with fear and uncertainty—long hospitalizations, unexpected complications, and the heartbreak of loss. Appropriate use of this technology will not only reduce the emotional toll on families but also alleviated the financial burden of prolonged hospital stays, which often strained already limited resources.
The healthcare providers were transformed- nurses and doctors gained confidence in the use of this life saving technology. Furthermore, the implementation of standardized guidelines is expected to enhance workflow efficiency, reduce healthcare costs and improve overall patient care and clinical outcomes.
Finally, the health system at large stood to benefit. Every neonate who survived without prolonged respiratory support freed up critical resources for other patients. Every staff member trained on the utilization of this low-cost technology, contributed to a growing cadre of healthcare workers skilled in neonatal care. The ripple effect extends beyond the SCBU: the model can be scaled to other neonatal units across the state and region, multiplying its impact over time
These projects proved that when we center interventions on people—the patients, families, and providers—meaningful, lasting change is possible.
