In January 2020, I will be returning with colleagues and faculty from Wake Forest to volunteer at Kijabe hospital for 4 weeks. There are no in-house radiologists at Kijabe. Normally, the studies are sent to Nairobi and there can be large delays in receiving image interpretations. Most of the clinicians at Kijabe have little faith in these radiologists, and usually interpret studies themselves. The leadership at Kijabe greatly appreciates our efforts and wants us to come as often as we can. Here is a summary of my previous trip.
We interpreted almost all of the hospitals CT scans. Wake Forest attending radiologists supervised the residents. We were consulted for x-rays, CT's and MRI's. Routinely we were asked for second opinions on studies performed well before our arrival. We also performed some imaged-guided procedures. The pathology in this region is very complex, and clinicians expressed gratitude for our more thorough reports and face-to-face interactions.
We worked intensively with the technologists to improve the quality of imaging and educate the staff in order to have a lasting effect. This included trouble-shooting CT protocols during the day and providing educational powerpoints to explain the reasoning for the protocols that we provided (adjusted for the limited resources available at Kijabe). The lead CT tech is sharing what he learned through a CME series with all of the technologists to ensure that protocols become more standardized going forward.
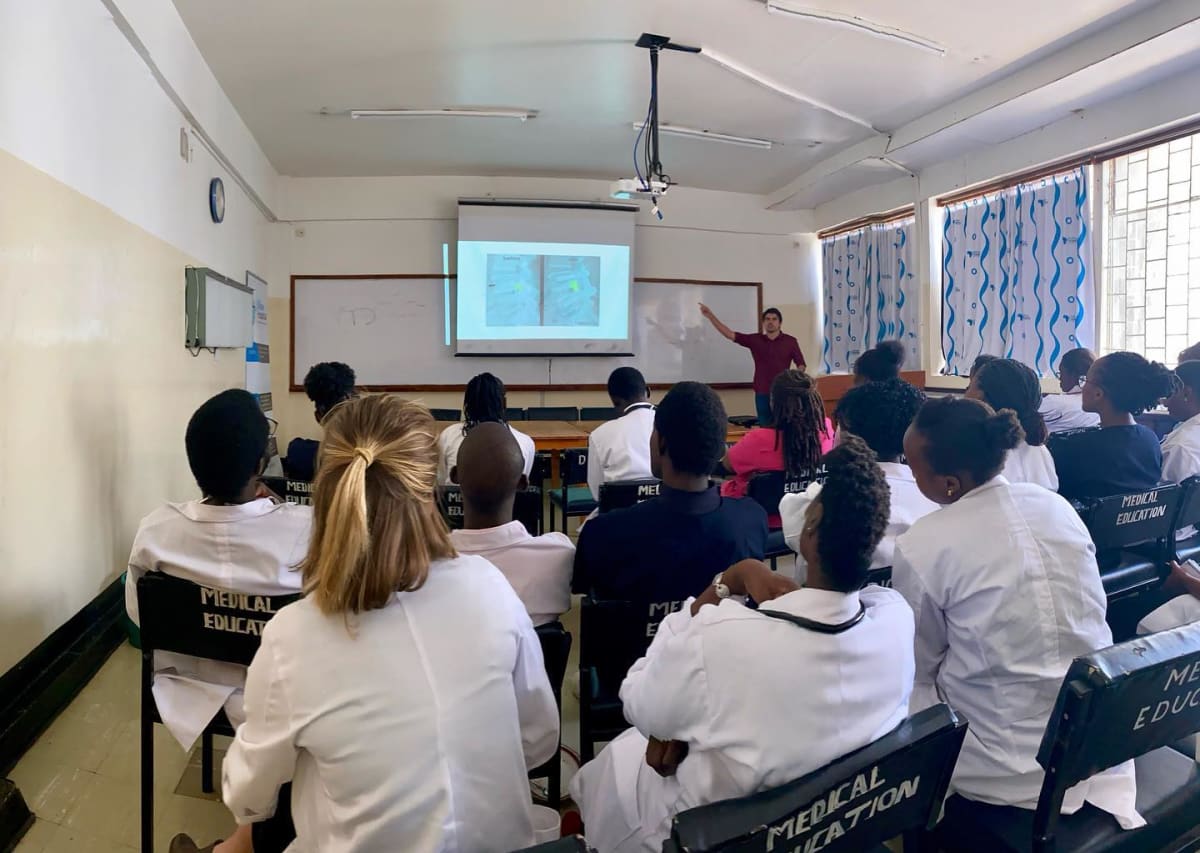
We taught CT, xray and ultrasound skills to house staff and gave them resources to study at home. We formally evaluated three residents that rotated with us. The physical therapy department also approached us, and we prepared three lectures at their request on the subject of spine and musculoskeletal imagine. I gave a body CT lecture and Cane gave a head CT lecture to the general house staff.
Contacts at Kijabe and I are planning specifics to build on this experience in 2020.
Kijabe is a regional hospital about an hour from Nairobi that serves a large region of surrounding Kenya. The patients are generally very poor, but have to pay out of pocket for medical care. Rather than expect perfection, they appreciate any and all efforts to help them. While originally staffed in large amount by visiting clinicians, the hospital relies on volunteers to employ a growing number of Kenyan clinicians and staff. The house staff also rely on volunteer lectures and daytime teaching from volunteers.
Wake Forest has been sending residents to Kijabe for over 5 years now. Our program director has been working to form an outline for formal global health rotations and is fully supportive of our efforts with help from our Chairman. Our ultimate goal is to collaborate with other institutions to provide Kijabe with year-round in-house radiology. Kijabe is open to providing permanent housing for radiology programs if we can guarantee a certain number of months covered. Multiple residents that went to Kijabe from Wake have also expressed interest in returning as adjunct faculty to oversee future mission trips.





















Kijabe is a small rural town over an hour away from Nairobi. The surrounding areas are extremely poor, and although Kijabe itself is considered nice, it also only has basic amenities and limited medical resources. Half of the hospital is transplanted and volunteer staff, while the other half are native Kenyans. People come into the hospital under extreme circumstances, because although the hospital is subsidized, the small patient costs are often still too high to bear. I've literally seen patients craw in on their hands and knees because they have chronic fractures that were never fixated. Strokes taking out nearly half the brain that began days or even weeks prior are the norm. Tumors grown out of control, nothing like what I've seen in four years of residency, are also commonplace. Despite the lack of access to care, the patients that do make it to the hospital are sincerely grateful for any help they can receive. Even when their loved ones pass, they extend gratitude for every healing effort and every action taken to make patients more comfortable. Here is a summary of what our team was doing in Kijabe.
After a couple long flights, we spent the night in Nairobi, bought some supplies, and headed out to Kijabe. We were oriented during the first day. We stayed in a very simple apartment that had basic amenities. Our work schedule included normal business hours during the weekdays, but we also stopped by the hospital numerous times at night and during the weekends at the requests of the clinicians and also to more generally review some of the cases performed while we were not present.
Chris Heald, Peter Zhang, Bhavana Budigi and I interpreted almost all of the hospitals CT scans and numerous ultrasounds during our time in Kijabe. We were supervised by Wake Forest radiologists. We were consulted by numerous physicians at the hospital, who brought hanging films of outside imaging for us to interpret because they questioned the reports provided from outside hospitals. These consults were for x-rays, CT’s and MRI’s. We also performed a handful of imaged-guided diagnostic and therapeutic procedures at the requested by the clinicians. The case difficulty was off the charts. Very few people go to the hospital in this area, and fewer have radiology studies performed. If someone gets a CT in Kijabe, it is going to be grossly positive, and research/review of articles is routinely necessary because the pathology is very different than what we see commonly at Wake Forest.
During our four weeks in Kijabe, we worked intensively with the technologists to improve the quality of imaging while we were there. More importantly, we prioritized educating the staff in order to create a lasting effect that would improve patient care in Kijabe year round. This work included trouble-shooting CT protocols during the day on a case by case basis, but also providing educational powerpoints explaining the reasoning for our specific protocols. We created extensive excel spreadsheets detailing protocols that we adjusted for the limited resources available at Kijabe. The lead CT tech is studying all of the resources we provided, and he plans to continue doing a CME series with all of the technologists to ensure that protocols become more standardized going forward.
The hospital assigned multiple family medicine residents to do a formal rotation under our supervision while we were in Kijabe. We tought basic CT, xray and ultrasound skills to these residents and gave them resources to study at home. We formally evaluated these residents, who all performed very well. We also gave more general lectures to the hospital house staff and pediatrics department. Lecture topics included chest, spine, pediatrics and ultrasound.
Before leaving, I gave the residents our information so that they could let us know which topics would be most helpful for next time. There is a good chance Dr. Heald will return next year to provide some continuity in our experience and teaching in Kijabe. I hope to return for a third time at some point to supervise residents. Clinicians at Kijabe have also kept in contact through WhatsApp and we have continued to offer consult services remotely on some of the more perplexing cases. Overall, the experience has provided us with profound perspective and has given us a greater appreciation for global health and we plan to integrate our experience and knowledge obtained during our time in Kenya into our practices here in the US.
