Interventional radiology (IR) is one of the newest recognized specialties in medicine. It’s importance and value stems from the ability to treat a wide range of conditions using minimally invasive techniques which has numerous safety advantages over more traditional invasive surgical options. Examples include image guided abscess drainage, nephrostomy and biliary tube placement, uterine fibroid embolization, and embolization in the setting of trauma, GI bleed, or postpartum hemorrhage. However, many low-income countries have limited or complete lack of IR services. According to the WHO over 4 billion people globally lack access to diagnostic imaging, with likely more than 5 billion lacking access to IR. As of 2017, there was not a single interventional radiologist in Tanzania, leaving a population equivalent to that of California and New York combined without access to a broad range of life-saving treatments.
I have been an attending IR physician at Duke University Hospital in Durham, NC for 31 years. I am the Program Director for the Integrated and Independent Interventional Radiology Residencies. I am also an Oral Boards Examiner for the American Board of Radiology. I had planned to travel to Tanzania two years ago. However, because of COVID, I taught the residents and prepared them for Oral Boards by Zoom platform instead over the last two years. I now would like to travel there in August of this year to perform Interventional Radiology cases with them and teach them in person. Many of our IR procedures are described in books, but an attending presence is necessary to cover the many technical details that are not included in the books. I also plan on examining them for their Oral Boards in August. One of the past trainees has begun a training program in Rwanda and I plan to visit his program in the future as well.
While this program most immediately serves the 60 million people living in Tanzania, training IR physicians locally will have regional impact. One of the first IR fellows who graduated with the first class in 2021 in Tanzania is from Rwanda, and has returned there as the first IR physician in the country. He has already begun the process of expanding these efforts there and plans to begin training the first generation of Rwandan IR trainees in late 2022. One of the prospective 2022 graduates in Tanzania is from Nigeria and will return there are completion of her training and start her own program in Nigeria. As such, our goal is to eventually serve the entire population of sub-Saharan Africa.
Expanding the many obvious benefits IR already provides to patients in high income nations can be quickly expanded to billions of people around the world in low-income nations by training young physicians locally. IR provides a broad range of life-saving procedures and can have an immediate impact, as has been demonstrated in Tanzania over the past several years. I want to support and expand these efforts and contribute to building IR services in Africa, potentially reaching over one billion people who currently have no access to these important treatments.






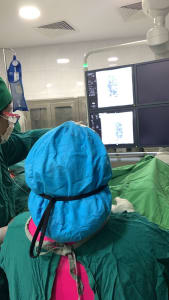

Our planned mission in Tanzania was two-fold. We wished to a) treat or help make diagnoses for the Tanzanian patients with minimally invasive procedures and to b) help train Tanzanian trainees in the arts of Interventional Radiology. Because of Covid, we had been teaching the trainees virtually on the Zoom platform and had also been preparing them for their Oral IR Boards. This was my first experience with meeting and training the residents in person with the help from a Doximity Grant.
We interviewed patients daily in the clinic with many disorders, including hepatocellular carcinoma, vascular malformations, mediastinal masses, uterine fibroids, renal obstruction, paraspinal tuberculous abscess, sigmoid diverticular abscess, biliary obstruction and renal cell carcinoma. These patients were later brought to the IR suite for drainage, ablation, embolization and biopsy procedures, using ultrasound and fluoroscopic guidance.
We also examined the IR residents for their IR Boards. Several International Boards examiners tested the residents on arterial procedures, venous procedures, non-vascular procedures and diagnostic IR imaging.
This was a wonderful experience that would not have been possible without help from Doximity. It became apparent that such a training program, with the help of international volunteers, can be sustainable as some graduates from the program have now stayed on as staff at the hospital to help train future IR physicians or have started IR training programs at institutions in neighboring countries.
